Case Report
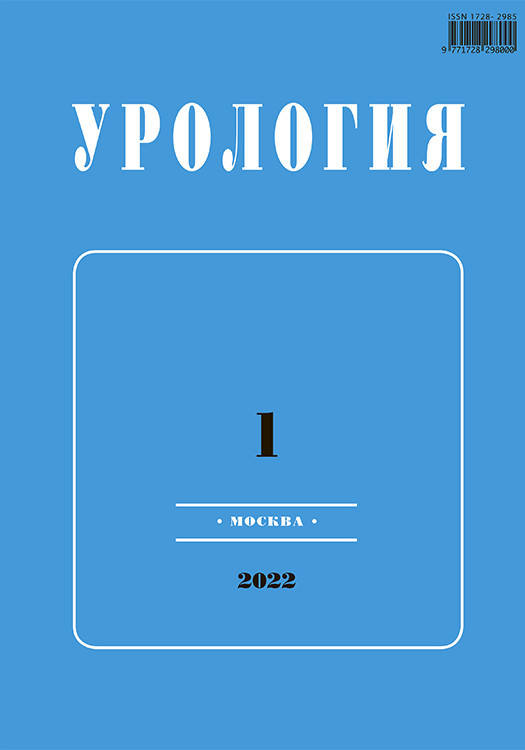
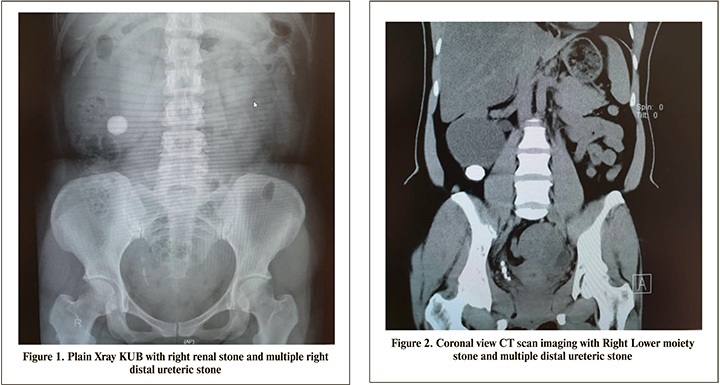
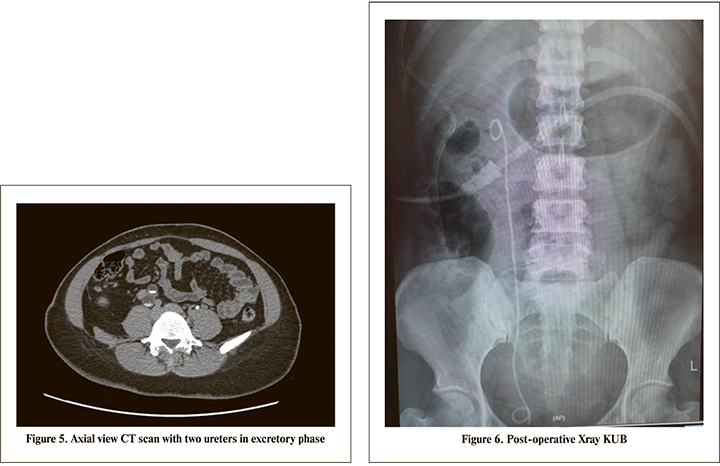
The patient is a 40 years old Malay lady presented with long history of right loin pain associated with radiating loin to groin pain with dysuria. Clinical examination showed no abdominal mass and bilateral kidneys were not ballotable with normal blood investigation results. An Xray KUB was done and showed right renal stone and multiple right distal ureteric stone (Figure 1). An ultrasound KUB performed and showed right hemorrhagic cyst with hydronephrosis. She had a non-contrast CT Kidney, ureter and bladder (KUB) performed and showed a lower moiety stone 1.6 cm x 2.3 cm with multiple distal ureteric stone with hydronephrosis and hydroureter (Figures 2,3 and 4). A CT Renal 4 phase was done and showed a right duplex with bifid ureters and obstructive uropathy due to distal ureteric stone and a right lower moiety renal calculus (Figure 5). She had a Diethylenetriamine pentaacetate (DTPA) scan and showed left kidney with 63.7% and right kidney 36.3% with upper moiety 85.4% and lower moiety 14.6% function. Subsequently a retrograde pyelogram and stenting was attempted but failed due to impacted distal ureteric stones. Hence, she was planned for primary Ureterorenoscopy (URS) and laser lithotripsy and laparascopic transperitoneal right heminephrectomy. Intraoperatively went smoothly and postoperative recovery was uneventful. Complete clearance of stones achieved (Figure 6). Her histopathology report confirmed features of non-functioning kidney with associated chronic inflammation. She was reviewed in the clinic 2 weeks postoperative for removal of stent and a subsequent clinic review with no signs of early and late complications.

Discussion
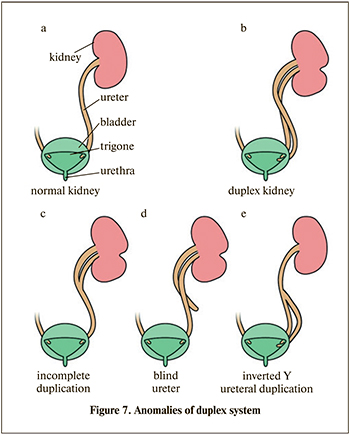
Renal duplex system are usually asymptomatic and identified incidentally. This anomaly are the most common variant of renal anatomy. Its incidence rate of 0.8% in healthy adult population and found in 2-4% of patients investigated for urinary tract symptoms [1]. Females are more commonly affected in 0.3% to 6% of the population. Importance of understanding this anomaly is to understand possible complications that may occur. Duplex system is defined as a kidney with 2 pyelocaliceal systems and associated as partial duplication with a single ureter or with a bifid ureter or complete duplication with 2 ureters that drains separately into the urinary bladder according to Weigert-Meyer Law (Figure 7) [2]. More commonly are unilateral duplication as compared to bilateral but having bilateral duplication is even rarer.
Urinary system develops from intermediate mesoderm. Around fifth week of development, the ureteric bud begins to appear from caudal end of mesonephric duct. The ureteric bud grows into nephrogenic cord and nephrogenic cord surrounds the ureteric bud forms the metanephric blastema. Cells from metanephric blastema will form nephrons which link to collecting tubules. The ureteric bud will form the kidney collecting system: collecting tubules, calyces, renal pelvis and ureter [3]. Common complications from this anomaly are obstruction, reflux disease and urinary stones or associated anomalies such as ureterocele and ectopic ureteric insertion [4].
Gold standard image modality for calculi is a non-contrast CT KUB. It has overtaken the role of CT Intravenous Uretherogram (IVU) in recent years. For this patient we had proceeded with CT kidney and excretory phase and proved of right kidney partial duplication system. Imaging is an important aspect and it gives a good visualization anatomy of right kidney and ureters to avoid misdiagnosis as abdominal cyst [5]. Therefore, it is important that duplex kidneys with hydronephrosis is considered in all patients with suspected abdominal cyst. Hence, patient had a URS and laser lithotripsy of calculi. It is reported to be an effective treatment modality for patients with symptomatic urolithiasis affecting a duplex collecting system. By understanding the anatomy, it prevented misleading to have normal URS during surgery as has been reported [6].
In a duplex kidney drained by double ureter, the lower moiety is more frequently affected compared to the upper pole due to coexisting complications since the lower moiety is dominant in most patients with renal duplex [7]. Patients usually present with loin pain, recurrent urinary tract infection or hematuria. This case occurred in the lower moiety with a preserved function of upper moiety. The observed obstruction in this patient must have been long standing causing destruction of parenchyma of the corresponding right lower renal moiety. Futher proven of non-functioning kidney by DTPA scan. Such late presentation with non-functioning corresponding renal moiety necessitating heminephrectomy has been reported [8]. Clement K. et al. done a systemic review and showed majority of cases requiring heminephrectomies for duplication of upper pole moiety. There were no data available for lower moiety heminephrectomy and considered to be a more complicated surgery in adults [9]. Hence, rarity and successful treatment for this patient.
Conclusion
Urinary system anomalies should go through thorough assessment with high suspicions by clinicians. Importance of understanding the anomalies is important. Imaging should be arranged accordingly and treatment should be individualized according to anatomy, duplication type and severity of obstruction to ensure good outcomes for patients.