Введение. Протяженные стриктуры мочеточников остаются сложной проблемой современной урологии. Основным методом их лечения являются различные реконструктивные операции на верхних мочевыводящих путях (ВМП), выбор которых в основном зависит от локализации и длины суженного участка [1, 2]. При стриктурах тазового отдела мочеточника применяются апробированные на достаточном клиническом материале операции Боари или psoas-hitch. В редких случаях по показаниям выполняется замещение мочеточника червеобразным отростком или сегментом подвздошной кишки [1, 3]. Иная ситуация наблюдается при протяженных стриктурах пиелоуретерального сегмента (ПУС) и проксимального отдела мочеточника, когда не представляется возможным выполнять резекцию с анастомозом «конец в конец». При сужениях данной локализации можно использовать реконфигурированный (операция Yаng–Monti) или тубулярный сегмент тонкой кишки, уретерокаликоанастомоз по Нейверту или аутотрансплантацию почки [1, 3–7]. Замещение мочеточника подвздошной кишкой – технически сложное вмешательство с высоким процентом осложнений, связанных с резекцией кишки, формированием межкишечного анастомоза и послеоперационными метаболическими изменениями. Выполнение анастомоза мочеточника с недостаточно расширенной нижней чашечкой и «толстой» паренхимой также может быть непростым и малоэффективным. Аутотрансплантация почки является сложным хирургическим вмешательством, ассоциированным с различными сосудистыми и урологическими осложнениями. Кроме того, эти операции, в отличие от реконструктивных вмешательств на тазовом отделе мочеточника, выполняются реже из-за сравнительно небольшого количества сужений проксимального участка мочеточника.
В связи с этим продолжается поиск новых технических решений. Одним из них является замещение дефекта проксимального участка мочеточника лоскутом из слизистой щеки. Данная методика хорошо зарекомендовала себя в реконструктивной хирургии стриктур уретры, и в литературе достаточно публикаций об удовлетворительных результатах этих операций [8–10]. Экспериментальные работы по замещению мочеточника буккальным графтом с хорошими результатами проводились еще в 1980-х гг. [11, 12]. Однако интерес практикующих урологов к этой методике вернулся в последнее десятилетие. В литературе имеются публикации о результатах пластики мочеточника буккальным лоскутом, выполненной открытым и робот-ассистированным доступами [13–19]. В основном в них приведены данные небольших серий пациентов или единичные наблюдения. Лапароскопическая буккальная уретеропластика выполнена только одному пациенту [20].
Цель исследования: изучить результаты лапароскопической пластики ПУС и проксимального отдела мочеточника лоскутом из слизистой щеки.
Материалы и методы. В Центре урологии Мариинской больницы лапароскопическая пластика протяженной стриктуры ПУС и верхней трети мочеточника буккальным лоскутом выполнена 10 больным, из них 7 мужчин. Средний возраст пациентов составил 43,5 (24–67) года.
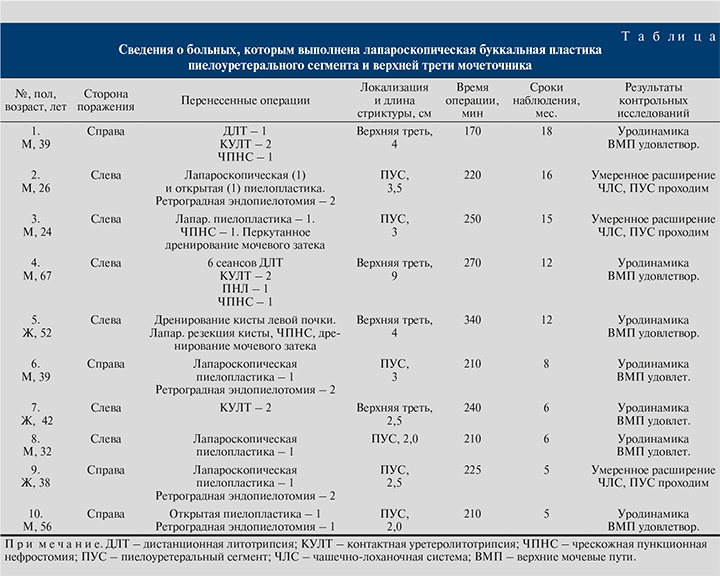
В 6 наблюдениях стриктура развилась после открытой или лапароскопической пиелопластики, в 3 – после контактной уретеролитотрипсии по поводу крупного камня верхней трети, в 1 – после лапароскопического иссечения кисты почки, осложнившегося травмой мочевых путей и затеком. Трое больных были госпитализированы в стационар с нефростомическим дренажем, семь – со стентом. У одного пациента после пиелопластики слева наряду с нефростомой был забрюшинный дренаж, установленный в связи с паранефральным затеком. Всем больным на предоперационном этапе выполняли ультразвуковое исследование почек, компьютерную томографию брюшной полости, антеградную пиелографию при наличии нефростомы и ретроградную уретерографию. Для уточнения функции пораженной почки проводилась динамическая сцинтиграфия. Сведения о пациентах представлены в таблице.
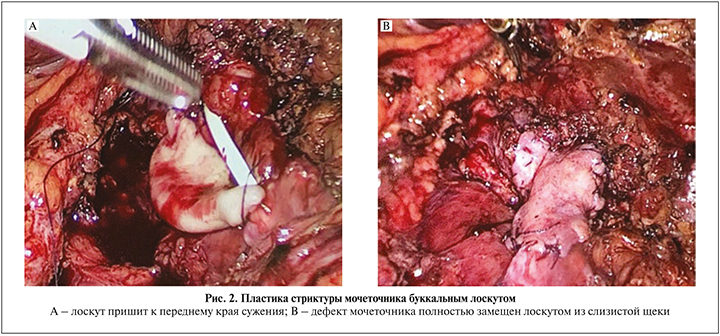
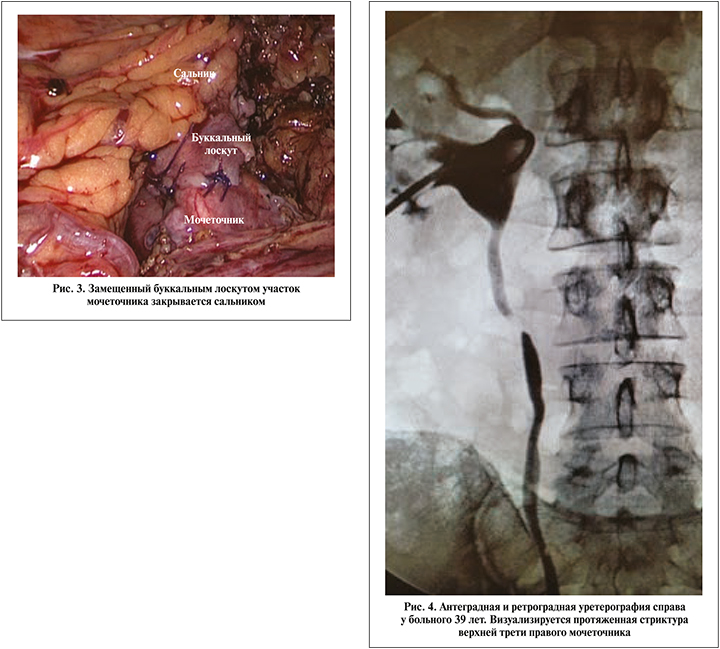
 Всем больным выполнена лапароскопическая пластика протяженной стриктуры ПУС и верхней трети мочеточника лоскутом из слизистой щеки. Операцию выполняли в положении на боку. Использовали 4 трокара, первый из которых устанавливали в подвздошной области по Хансону. После инсуфляции брюшной полости до 12 мм рт.ст. проводили еще три троакара: два по 6 мм по подключичной линии в подвздошной области и ниже реберной дуги, один 6 мм по задней аксиллярной линии. Далее мобилизовали толстую кишку и отводили ее медиально. С иссечением рубцовых тканей в забрюшинном пространстве идентифицировали мочеточник на протяжении верхней трети. Максимально сохраняя неизмененные ткани, выделяли мочеточник выше и ниже сужения. При стриктуре ПУС проводили адекватную мобилизацию лоханки. Далее рассекали мочеточник на протяжении суженного участка и на 1 см выше и ниже этой зоны. При обструкции ПУС разрез продолжали проксимальнее на лоханку. Протяженность стриктуры мочеточника определяли с помощью мочеточникового катетера, заведенного в брюшную полость (рис. 1). После этого осуществляли забор слизистой щеки соответствующей длины, дефект ее ушивали непрерывным швом. Далее лоскут подготавливали к пластике и через троакар проводили в брюшную полость. Несколькими узловыми швами фиксировали его к дистальному и проксимальному краям суженного участка мочеточника, что облегчало дальнейшее наложение швов. Вначале непрерывный шов (викрил 4/0) накладывали между буккальным лоскутом и передним краем мочеточника, антеградно устанавливали стент 7 Шр и ушивали заднюю стенку (рис. 2). Герметичность швов проверяли путем наполнения лоханки стерильным раствором через нефростомический дренаж, при необходимости накладывали дополнительные узловые швы. Далее буккальный лоскут окутывали сальником, который фиксировали к мочеточнику несколькими узловыми швами (рис. 3). В зону операции устанавливали дренаж, троакары извлекали, раны ушивали.
Всем больным выполнена лапароскопическая пластика протяженной стриктуры ПУС и верхней трети мочеточника лоскутом из слизистой щеки. Операцию выполняли в положении на боку. Использовали 4 трокара, первый из которых устанавливали в подвздошной области по Хансону. После инсуфляции брюшной полости до 12 мм рт.ст. проводили еще три троакара: два по 6 мм по подключичной линии в подвздошной области и ниже реберной дуги, один 6 мм по задней аксиллярной линии. Далее мобилизовали толстую кишку и отводили ее медиально. С иссечением рубцовых тканей в забрюшинном пространстве идентифицировали мочеточник на протяжении верхней трети. Максимально сохраняя неизмененные ткани, выделяли мочеточник выше и ниже сужения. При стриктуре ПУС проводили адекватную мобилизацию лоханки. Далее рассекали мочеточник на протяжении суженного участка и на 1 см выше и ниже этой зоны. При обструкции ПУС разрез продолжали проксимальнее на лоханку. Протяженность стриктуры мочеточника определяли с помощью мочеточникового катетера, заведенного в брюшную полость (рис. 1). После этого осуществляли забор слизистой щеки соответствующей длины, дефект ее ушивали непрерывным швом. Далее лоскут подготавливали к пластике и через троакар проводили в брюшную полость. Несколькими узловыми швами фиксировали его к дистальному и проксимальному краям суженного участка мочеточника, что облегчало дальнейшее наложение швов. Вначале непрерывный шов (викрил 4/0) накладывали между буккальным лоскутом и передним краем мочеточника, антеградно устанавливали стент 7 Шр и ушивали заднюю стенку (рис. 2). Герметичность швов проверяли путем наполнения лоханки стерильным раствором через нефростомический дренаж, при необходимости накладывали дополнительные узловые швы. Далее буккальный лоскут окутывали сальником, который фиксировали к мочеточнику несколькими узловыми швами (рис. 3). В зону операции устанавливали дренаж, троакары извлекали, раны ушивали.
В послеоперационном периоде проводили антибактериальную и инфузионную терапию. После извлечения дренажа пациентов выписывали на амбулаторное лечение с нефростомой и стентом. Стент удаляли через 6 нед., выполняли антеградную пиелоуретерограмму, экскреторную урографию или КТ брюшной полости с внутривенным контрастированием, динамическую сцинтиграфию.
Результаты. Все операции были успешно выполнены лапароскопическим доступом. Интраоперационных осложнений не было, гемотрансфузии не проводились. Длительность операций колебалась от 170 до 340 мин, основное время (110–180 мин) занимало иссечение послеоперационных рубцов и мобилизация мочеточника. Продолжительность госпитализации составила 5–6 дней. Случаев подтекания мочи по дренажу не было. Лихорадка до 38,0°С наблюдалась у одного пациента без нефростомического дренажа (I степень по Клавьену). Осложнений по Клавьену III степени и выше не было.
Клинически все операции признаны успешными, так как удалось избавить пациентов от нефростомического дренажа и внутреннего стента. По данным экскреторной и КТ урографии участок мочеточника, замещенный буккальным лоскутом, был широким и хорошо проходимым. У пациентов со стриктурами ПУС в динамике наблюдалось уменьшение размеров чашечек и лоханки, но расширение полностью не исчезало. При стриктурах проксимального участка мочеточника уродинамика ВМП была удовлетворительной.
Приводим клиническое наблюдение успешной лапароскопической буккальной пластики верхней трети правого мочеточника.
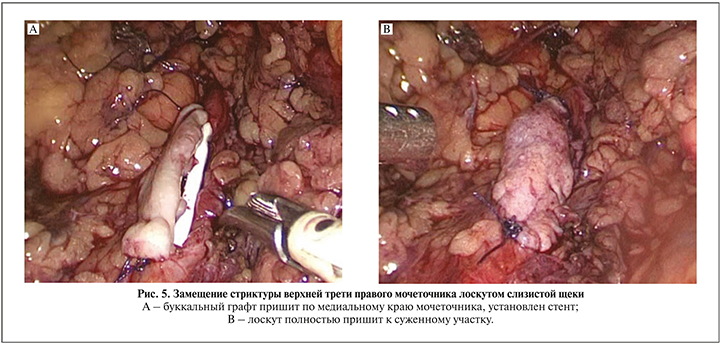
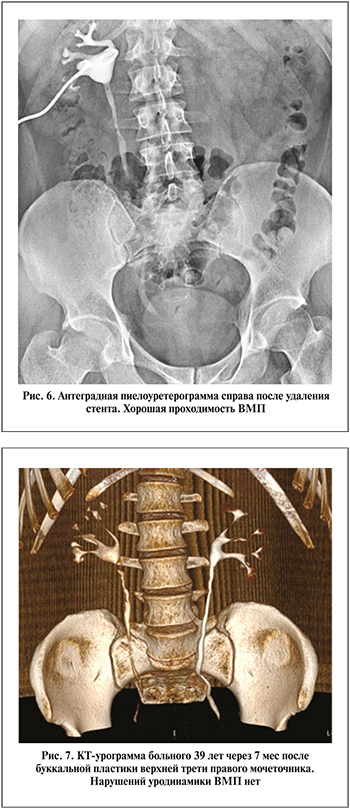 Больной Б. 39 лет 09.07.2019 госпитализирован в клинику с диагнозом «стриктура верхней трети правого мочеточника, нефростома справа». Из анамнеза известно, что в декабре 2018 г. был в экстренном порядке госпитализирован с диагнозом «мочекаменная болезнь, камень средней трети правого мочеточника, почечная колика справа». При обследовании выявлен рентген-позитивный камень размером примерно 11 мм. Установлен стент, проведено два сеанса дистанционной литотрипсии без положительного эффекта. В январе 2019 г. в плановом порядке выполнена контактная лазерная уретеролитотрипсия справа, после которой часть камня мигрировала в чашечно-лоханочную систему. По этой причине вновь установлен стент и пациент выписан на амбулаторное лечение. В марте 2019 г. повторная госпитализация, в ходе которой выполнена лазерная контактная литотрипсия, конкремент полностью фрагментирован и удален. В апреле 2019 г. мочеточниковый стент извлечен. Однако через месяц вновь развился приступ почечной колики, при КТ брюшной полости с контрастированием данных за камень мочеточника не получено, выявлена стриктура верхней трети правого мочеточника. При диагностической уретероскопии на этом уровне выявлена облитерация. Выполнена перкутанная нефростомия справа. При антеградной пиелографии и ретроградной уретерографии визуализировалась протяженная стриктура проксимальной части правого мочеточника длиной около 3 см (рис. 4). 09.07.2019 в нашей клинике выполнена лапароскопическая буккальная пластика верхней трети правого мочеточника по вышеописанной методике (рис. 5). Длительность операции составила 180 мин, кровопотеря – 50 мл. Осложнений не было, дренаж удален на 3-е сутки и на 6-й день выписан на амбулаторное лечение. Стент извлечен через 6 нед. При антеградной пиелографии и по данным КТ проходимость правого мочеточника хорошая, нарушений уродинамики нет (рис. 6, 7). В течение периода наблюдения (8 мес.) состояние пациента стабильное, жалоб нет.
Больной Б. 39 лет 09.07.2019 госпитализирован в клинику с диагнозом «стриктура верхней трети правого мочеточника, нефростома справа». Из анамнеза известно, что в декабре 2018 г. был в экстренном порядке госпитализирован с диагнозом «мочекаменная болезнь, камень средней трети правого мочеточника, почечная колика справа». При обследовании выявлен рентген-позитивный камень размером примерно 11 мм. Установлен стент, проведено два сеанса дистанционной литотрипсии без положительного эффекта. В январе 2019 г. в плановом порядке выполнена контактная лазерная уретеролитотрипсия справа, после которой часть камня мигрировала в чашечно-лоханочную систему. По этой причине вновь установлен стент и пациент выписан на амбулаторное лечение. В марте 2019 г. повторная госпитализация, в ходе которой выполнена лазерная контактная литотрипсия, конкремент полностью фрагментирован и удален. В апреле 2019 г. мочеточниковый стент извлечен. Однако через месяц вновь развился приступ почечной колики, при КТ брюшной полости с контрастированием данных за камень мочеточника не получено, выявлена стриктура верхней трети правого мочеточника. При диагностической уретероскопии на этом уровне выявлена облитерация. Выполнена перкутанная нефростомия справа. При антеградной пиелографии и ретроградной уретерографии визуализировалась протяженная стриктура проксимальной части правого мочеточника длиной около 3 см (рис. 4). 09.07.2019 в нашей клинике выполнена лапароскопическая буккальная пластика верхней трети правого мочеточника по вышеописанной методике (рис. 5). Длительность операции составила 180 мин, кровопотеря – 50 мл. Осложнений не было, дренаж удален на 3-е сутки и на 6-й день выписан на амбулаторное лечение. Стент извлечен через 6 нед. При антеградной пиелографии и по данным КТ проходимость правого мочеточника хорошая, нарушений уродинамики нет (рис. 6, 7). В течение периода наблюдения (8 мес.) состояние пациента стабильное, жалоб нет.
В представленном клиническом наблюдении неоднократные эндоскопические вмешательства привели к формированию протяженной стриктуры проксимального отдела мочеточника. При сужениях данной локализации методом выбора может быть замещение реконфигурированным сегментом тонкой кишки по Yang–Monti. Однако данное вмешательство технически непростое, и буккальная пластика мочеточника стала эффективной альтернативой, позволившей восстановить проходимость ВМП.
Обсуждение. Протяженные стриктуры ПУС и проксимального отдела мочеточника являются сложной урологической нозологией, требующей проведения различных реконструктивных вмешательств. Выполнить анастомоз «конец в конец» без натяжения в этих случаях не всегда получается, поэтому применяются такие вмешательства, как уретерокаликоанастомоз, пластика мочеточника реконфигурированным сегментом тонкой кишки по Yang–Monti и аутотрансплантация почки [1, 3–7]. Операция Нейверта подразумевает резекцию части паренхимы почки над нижней чашечкой для анастомозирования с мочеточником. Недостаточное удаление паренхимы и плохое сопоставление слизистых нижней чашки и мочеточника приводят к обструкции ВМП и неудовлетворительным результатам [7]. Пластика по Yang–Monti требует проведения резекции небольшого участка тонкой кишки, его реконфигурации в виде трубки на брыжейке и выполнения анастомозов с проксимальным и дистальным концами мочеточника. Для аутотрансплантации почки необходимы определенные технические навыки в трансплантации, после нее наблюдаются псевдоаневризмы и тромбоз почечной артерии [4, 5]. В связи с этим продолжается поиск менее сложных и высокоэффективных реконструктивных вмешательств на мочеточнике. В прошлом веке было проведено много экспериментальных исследований по замещению мочеточника аутовеной, червеобразным отростком, маточной трубой и лоскутом из слизистой щеки. Из этих материалов в редких случаях используется аппендикс для пластики нижней и средней третей правого мочеточника [1, 3].
Буккальный лоскут активно используется при пластике уретры [8–10]. Он легко доступен для изъятия, менее подвержен отторжению и хорошо подходит для замещения мочевыводящих путей. Экспериментальные работы по замещению мочеточника слизистой щеки на обезьянах были выполнены в 1983 г. [11, 12]. После резекции мочеточника в средней трети около 3 см из лоскута слизистой щеки формировали трубку, которой замешали дефект мочеточника. Последующее кровоснабжение зоны операции обеспечивали окутыванием сальником. Гистологические исследования подтвердили хорошую васкуляризацию лоскута, а на урограммах наблюдалась адекватная проходимость ВМП [11, 12]. Уретеропластика слизистой щеки у 6 пациентов впервые была выполнена J. H. Naude [21]. У 4 пациентов суженный участок мочеточника рассекали и пришивали буккальный лоскут, в одном случае выполнена аугментационная буккальная пластика анастомоза мочеточника, еще в одном – его замещение тубулярным лоскутом. Во всех случаях зону операции окутывали сальником. За период наблюдения 24 (2–72) мес. рецидивов сужения не было, дополнительные вмешательства не проводились.
В литературе имеются единичные публикации о результатах буккальной пластики мочеточника открытым и эндовидеохирургическим доступами [13–19]. По данным авторов, выполнявших подобные реконструктивные операции, основным показанием к буккальной уретеропластике были рецидивные стриктуры проксимального отдела мочеточника. При данном вмешательстве необходимо выделить его из рубцовых тканей только на протяжении суженного участка, выполнить его инцизию и пришить буккальный лоскут. У пациентов с облитерацией просвета измененную зону можно резецировать и выполнять аугментационную анастомотическую буккальную пластику. Результаты открытой пластики мочеточника слизистой оболочкой щеки описаны несколькими авторами [13–15]. D. Kroepfl et al. [13] выполнили данное вмешательство 6 больным со стриктурами средней и нижней третей мочеточника по методике onlay. У одного больного процесс был двусторонний. Протяженность стриктур варьировалась от 3 до 11 см, составив в среднем 7 см. За период наблюдения, 18 (10–85) мес., у 5 (71,4 %) больных обструкции ВМП не было. Двум пациентам с рецидивом стриктуры через 17 и 30 мес. соответственно проведена пункционная нефростомия. А. А. Badawy et al. [14] выполнили тубулярную буккальную уретеропластику 5 пациентам с сужениями проксимального отдела мочеточника средней длиной 4,5 (3,5–5) см. При резекции измененного участка адвентицию по возможности сохраняли и использовали для дополнительной васкуляризации графта. За период наблюдения 18 (14–26) мес. у всех пациентов подтверждена адекватная проходимость на урограммах. Несмотря на обнадеживающие результаты тубулярной буккальной уретеропластики, имеются разногласия по использованию этой техники. Так, оnlay и тубулярная пластика слизистой щеки ассоциируются с рецидивом сужения мочеточника, частота которого достигает 11 и 45% соответственно, что связано с недостаточной васкуляризацей лоскута [14, 22]. Однако не следует полностью отказываться от тубулярной пластики и необходимо дальнейшее проведение работ, сравнивающих результаты тубулярной и onlay-буккальной уретеропластики.
Все последние работы посвящены результатам робот-ассистированной буккальной уретеропластики [16–19].
L. C. Zhao et al. [16] роботическую пластику слизистой щеки выполнили 4 пациентам со стриктурами проксимального отдела мочеточника со средней длиной 4 (1,5–6) см.
Верхний и дистальный края сужения они определяли с помощью гибкой уретероскопии с иммунофлюоресцентной визуализацией. При облитерации мочеточника и невозможности проведения уретероскопа внутривенно вводили индоцианин зеленый, который окрашивал хорошо перфузируемую ткань мочеточника в зеленый цвет, а суженный участок при этом оставался темным. Эффективность оценивали с помощью УЗИ и реносканирования. При среднем сроке наблюдения 15,5 (10,7–18,6) мес. данных за рецидив не получено. S. Arora et al. [17] также использовали гибкую уретероскопию и иммунофлюоресцентную визуализацию для определения дистальной части сужения длиной 6 см у больного, которому ранее неудачно был выполнен роботический уретеролиз. За 6-месячный период наблюдения данных за рецидив сужения не получено. Z. Lee et al. [18] выполнили робот-ассистированную буккальную уретеропластику 12 пациентам с стриктурами проксимального отдела мочеточника, у 8 из которых они были рецидивными. Средняя длина мочеточника была равна 3 (2–5) см. Они также использовали иммунофлюресцентную визуализацию для уточнения границ суженного участка. Во всех случаях оперированный участок мочеточника окутывался сальником. За период наблюдения (13 мес.) результаты операции у 10 (83,3%) больных были клинически и радиологически хорошими. L. C. Zhao et al. [23] опубликовали результаты робот-ассистированной буккальной уретеропластики, выполненной 19 больным в трех клиниках США. В 74% случаев стриктура локализовалась в верхней трети, в 26% – в средней трети, протяженность составила 4 (2–8) см.
В отношении 79% больных была использована onlay-методика, в отношении остальных – аугментационная техника анастомоза. За средний период наблюдения (26 мес.) общий процент успеха составил 90.
В литературе имеется единственное описание лапароскопической буккальной уретеропластики, выполненной 42-летнему мужчине со стриктурой верхней трети мочеточника длиной 3 см после контактной уретеролитотрипсии [19]. Данную операцию мы выполнили у 10 больных с рецидивными стриктурами проксимального мочеточника со средней длиной 3,8 см. Наибольшая длина суженного участка составила 9 см, в данном случае мы столкнулись с трудностями при выкраивании лоскута адекватной длины. У остальных пациентов протяженность стриктуры была меньше 4 см, и подобных проблем не возникало. Двумя лоскутами можно заместить более длинные сужения мочеточника. Однако, на наш взгляд, в подобных ситуациях целесообразно использовать более сложные, но эффективные и надежные способы реконструкции, например пластику тонкой кишки по Yang Monti. По сравнению с ней уретеропластика слизистой щеки менее сложна и имеет низкий процент осложнений. В связи с этим данная операция на первый взгляд кажется привлекательной и простой в исполнении. Однако необходимы дальнейшее накопление опыта и мультиклинические исследования для уточнения роли буккальной уретеропластики в реконструктивной хирургии мочеточника.
Заключение. Протяженные стриктуры проксимального отдела мочеточника служат показанием к таким реконструктивным операциям, как кишечная пластика или аутотрансплантация почки. Эти операции относятся к категории сложных вмешательств, выполняемых в крупных урологических клиниках с достаточным опытом в реконструктивной хирургии ВМП. Пластика длинной стриктуры ПУС и проксимального отдела мочеточника лоскутом из слизистой щеки является менее сложной, но высокоэффективной операцией. Для хорошего результата необходимы мобилизация суженного участка мочеточника, рассечение его по передней поверхности до здоровых проксимального и дистального участков, замещение буккальным графтом. При его неэффективности методом выбора может быть илеоуретеропластика по Yang–Monti.